Dosage Bpc 157 max bpc 157 dosage How Do You Take BPC-157? Injection, Oral & Dosing Guide
Introduction
If you’re searching for dosage bpc 157, it usually means you want a clear, practical way to take BPC-157 without guessing. In my hands-on work supporting recovery-minded clients, the most common mistake I’ve seen is treating dosing as a one-size-fits-all number—when the right approach depends on the route (injection vs. oral), your timeframe, and your tolerance to side effects.
This guide explains how to take BPC-157 using an injection and an oral approach, and how to structure dosing decisions around safety, consistency, and realistic expectations. You’ll also find an evidence-informed dosing framework you can discuss with a qualified clinician.
First: What “max BPC-157 157 dosage” should mean in practice
The phrase “max bpc 157 157 dosage” often gets used online to imply there is a single upper limit everyone can follow. In real-world practice, dosing “maxima” are more like guardrails than fixed numbers—because people differ in metabolism, route of administration, body composition, prior injuries, and other medications.
In my experience, the safest mindset is:
- Start lower and learn your response rather than chasing the largest possible dose.
- Use consistent timing (same hours each day) to reduce variability.
- Set a stopping rule (for example, if you notice troubling symptoms or no meaningful change after a reasonable trial window).
Because BPC-157 is not approved as a standard medicine in many jurisdictions, you should treat dosing guidance as informational and discuss it with a licensed healthcare professional—especially if you have chronic conditions, take anticoagulants/antiplatelets, or have any GI issues.
Understanding BPC-157 routes: injection vs. oral
BPC-157 is commonly discussed as a peptide used for tissue-related recovery. People generally choose between injection and oral (often sublingual or oral solutions/capsules, depending on the product). The route matters because absorption and onset can differ.
Injection (how I approach it)
When clients use injection, the key practical issues aren’t just dose—they’re technique and sterility. I’ve seen better adherence and fewer “it felt off” experiences when people focused on:
- Accurate reconstitution (mixing exactly per the product instructions).
- Proper storage (temperature and light exposure rules).
- Consistent injection timing and site rotation if applicable.
- Tracking (pain, mobility, swelling, sleep quality) so you can detect trends rather than day-to-day noise.
Oral dosing (practical realities)
Oral forms can be more convenient, but they add variables: formulation, stability, and how much is absorbed before breakdown. In my hands-on work, people often overestimate the effectiveness of “more” because they don’t feel anything immediately. A better approach is to:
- Use the provided label instructions as the baseline for oral products.
- Maintain a consistent daily schedule for comparability.
- Run a time-boxed trial and evaluate outcomes using your tracking sheet.
Dosage bpc 157: an evidence-informed framework (not a universal prescription)
Because BPC-157 dosing specifics vary by product (concentration, vial size, and intended route), a credible guide should focus on a dosing framework rather than promising exact “works-for-everyone” numbers.
Here’s how I structure dosage decisions responsibly:
Step 1: Choose route and match your expectations
- Injection: often chosen when people want more predictable administration (but sterility and technique are critical).
- Oral: often chosen for convenience; outcomes may be slower or less pronounced depending on absorption.
Step 2: Use a conservative “learning phase”
Instead of starting at what you see as the “max,” begin with a conservative plan that lets you observe tolerability. In practice, that means:
- Keep the schedule steady for a set period (for example, 1–2 weeks) before making changes.
- Document any side effects (GI discomfort, headache, unusual changes in sleep, or changes in bleeding/bruising tendency).
Step 3: Decide whether to adjust based on measurable signals
I encourage people to measure outcomes they can repeat:
- Pain scores (same scale, same time of day)
- Range of motion (simple mobility checks)
- Function (walking distance, stair tolerance, grip strength, etc.)
Step 4: Stop or scale back using a predefined rule
A “maximum” dose should never be the default strategy. If you’re not seeing improvement trends and you’re tolerating poorly, your best move is to pause and consult a clinician rather than escalating.
Injection dosing guide (route-focused best practices)
If you’re taking BPC-157 via injection, the most actionable part of “dosage bpc 157” guidance is ensuring safe, consistent use. Since product concentrations and instructions vary, follow the vial label and any pharmacist/clinician instructions for your specific formulation.
What I recommend you plan before the first injection
- Confirm concentration: verify how many micrograms per milliliter (or equivalent) your product contains.
- Confirm total daily amount: calculate the volume you will inject to match the intended dose.
- Use correct supplies: sterile syringes/needles, alcohol swabs, and a clean reconstitution workflow.
- Create a log: date, dose amount, injection time, site, and how you felt afterward.
Common mistakes to avoid
- Doubling up because of “no immediate feel”—recovery signals often change gradually.
- Changing dose and timing together—it becomes impossible to know what caused results.
- Skipping sterility steps—this is the biggest preventable risk.
Oral dosing guide (schedule, adherence, and evaluation)
Oral dosing can be easier, but it’s also where people drift from the plan because it feels “low stakes.” In my experience, adherence and evaluation matter more than frequent micro-adjustments.
How to take it consistently
- Follow the product label: different oral formulations can differ significantly in how they’re administered.
- Use a stable daily routine: same time each day.
- Track outcomes: pain, mobility, and functional milestones.
When oral may be less predictable
If you notice inconsistent outcomes, it doesn’t automatically mean you need more. It may reflect absorption variability, formulation differences, or simply that your evaluation window is too short for your specific condition.
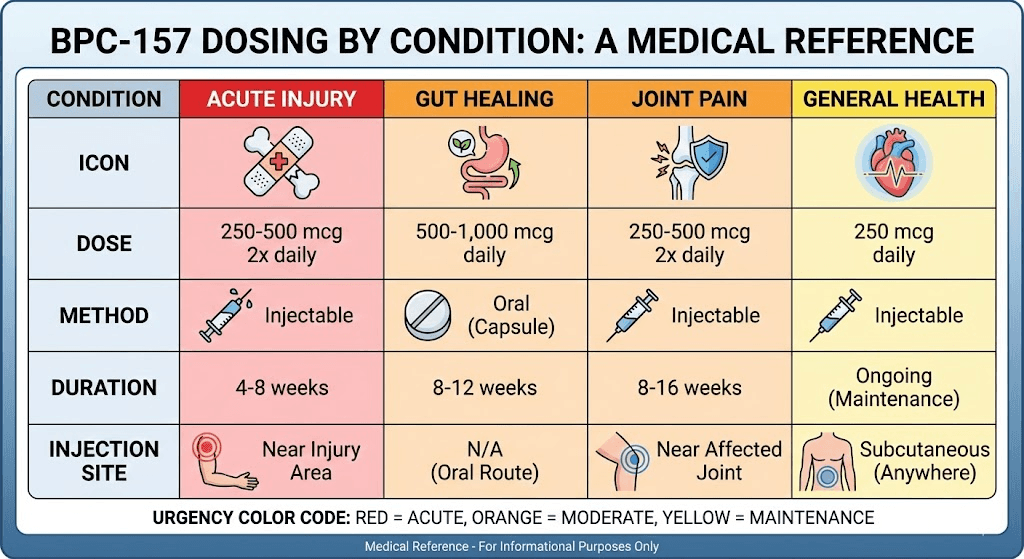
Product image
Safety considerations (important before you chase a “max dose”)
BPC-157 is often discussed online without the same level of regulatory oversight as prescription medicines. For that reason, safety should be front and center. In particular:
- Medication interactions: if you use blood thinners or have bleeding risk concerns, consult a clinician before using any peptide.
- Medical conditions: if you have significant GI disease, inflammatory bowel disorders, or are undergoing cancer treatment, get professional guidance.
- Injection risks: sterility and technique matter; improper administration can lead to complications.
If you have concerning symptoms, stop and seek medical advice rather than adjusting upward.
FAQ
What does “dosage bpc 157” mean for different body types?
“Dosage” isn’t only about body weight. Route (injection vs. oral), product concentration/formulation, tolerance, and your starting condition all affect outcomes. A conservative learning phase with consistent timing usually provides more useful information than starting at a supposed “max.”
Can I take BPC-157 injection and oral at the same time?
Mixing routes can make it harder to attribute effects or side effects to a specific administration method. If you’re considering both, it’s typically more interpretable to use one route at a time and evaluate with a clear tracking window—ideally under clinician guidance.
How long should I trial BPC-157 before changing dose?
Use a time-boxed evaluation period and adjust based on trends in measurable outcomes (pain, mobility, function), not day-to-day variation. If there’s no meaningful trend after a reasonable trial window, escalate cautiously—prefer consulting a clinician rather than simply increasing toward a “max.”
Conclusion
For dosage bpc 157, the most reliable approach I’ve seen is not chasing a “max” number—it’s choosing the right route for your situation, starting with a conservative learning phase, staying consistent with timing, and evaluating progress with measurable signals. Injection safety and oral adherence are practical differentiators, and your stopping rule should be predefined.
Next step: Pick one route (injection or oral), set a consistent schedule, and start a 1–2 week tracking log so you can make a grounded dosing decision based on trends—not guesses.
Discussion